
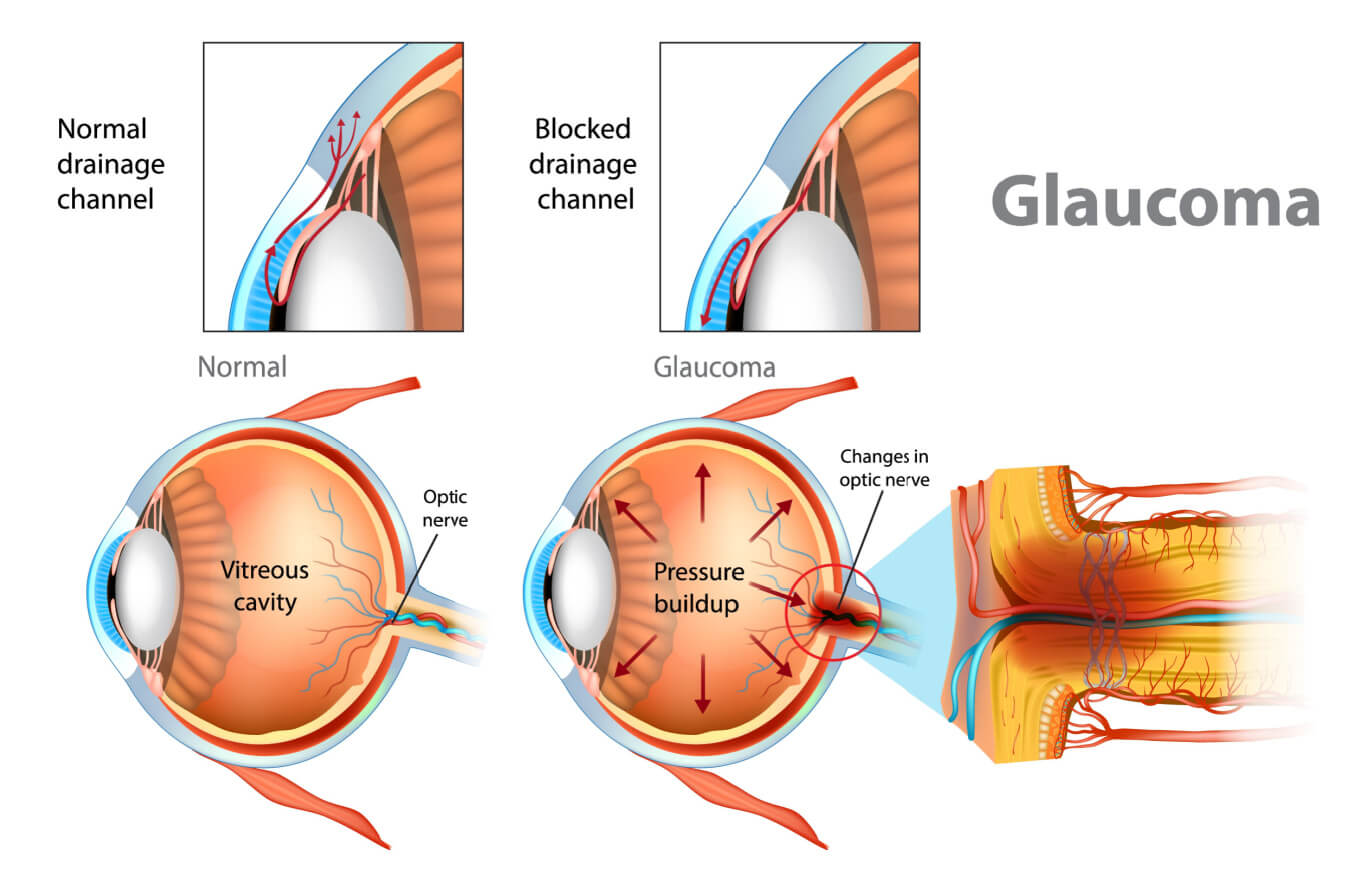
Inverted poses are important in Iyengar yoga. Senior practitioners often cite an inversion as their most essential pose. (Sarvangasana (shoulderstand) seems to be a favorite.) Can anyone do inversions? General contraindications include spinal disorders, hypertension, and glaucoma. Recently, however, I’ve met yoga students with glaucoma who do brief inversions with the approval of their ophthalmologists. Hmm…
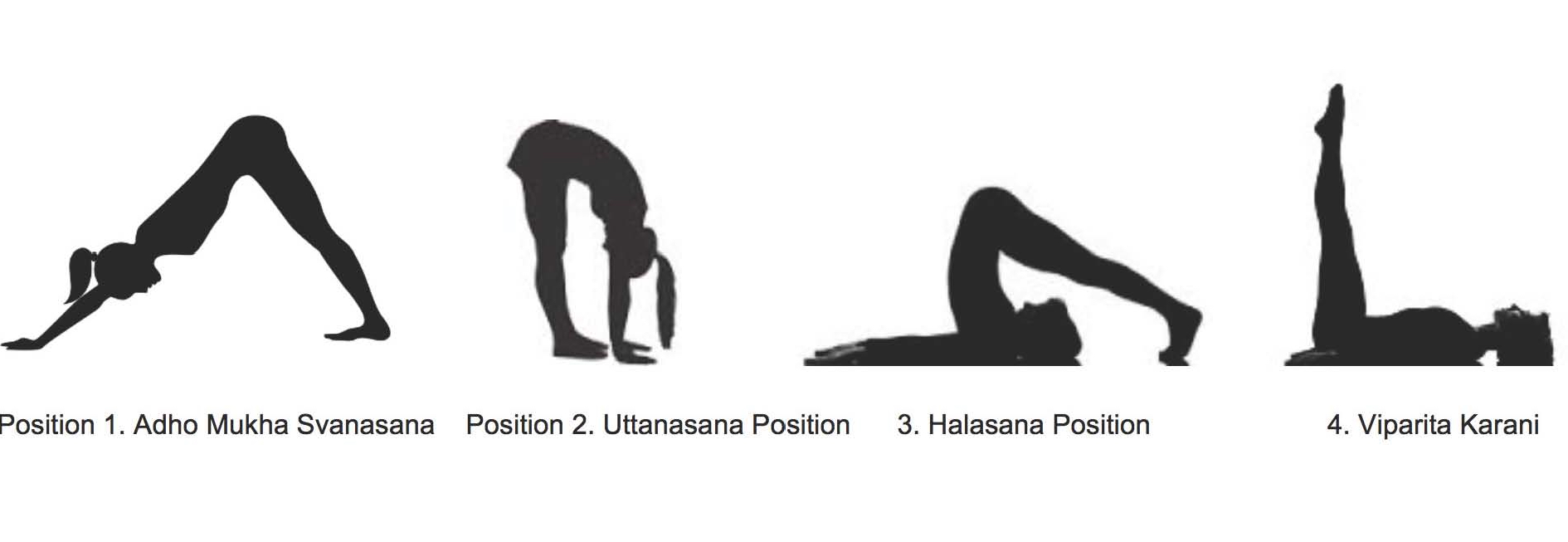
Around the same time, I read a PLOS ONE study published in December 2015 that measured intraocular pressure (IOP) in 10 subjects with primary open-angle glaucoma and 10 normal subjects during the following poses, each done for two minutes: Adho Mukha Svanasana, Uttanasana, Halasana, Viparita Karani. The researchers opted not to study Sirsasana (headstand) to see if less-inverted poses also affect IOP.
In both normal and glaucoma subjects, the following occurred:
- IOP increased in all non-upright body positions. Pressures increased within one or two minutes after entering a pose. Likewise they returned to baseline values a few minutes after exiting the pose. (The prompt “return to baseline” is apparently one reason why ophthalmologists allow glaucoma patients to do inversions.)
- IOP change is directly related to body angle from upright to inverted.
- Among the four study poses, Adho Mukha Svanasana caused the greatest increase, followed by Uttanasana, Halasana, and Viparita Karani.
- IOP remains elevated while non-upright position is maintained.
- Glaucoma subjects did not show more severe IOP increases than normal subjects. Both groups showed a rise in IOP between 6-11 mmHg.
Note: Limitations of this study include small sample size, short pose duration, no measurement of blood pressure, and age variation between glaucoma and normal groups.
What the study could not (and did not) answer: Are temporary IOP increases safe for glaucoma patients?
I solicited my own eye doc’s opinion, and he was wary of inversions for glaucoma patients. He prefers not to take chances with possible optic nerve damage. A few minutes of elevated pressure day after day, he hypothesized, adds up over the years. Loren Fishman, MD, prominent specialist in physical medicine and rehabilitation and longtime Iyengar yoga practitioner, considers inversions beneficial for those without contraindications—but advises glaucoma patients to weigh the risks of increased IOP, even if temporary. In a 2013 New York Times interview, he said, ” I believe headstand and handstand are contraindicated by wide angle and narrow angle glaucoma.”
In the mid 2000s, Fishman, then a 67-year-old male without glaucoma, held Salamba Sirsasana and variations for 21 minutes in a self-administered study (link currently invalid). During this time, his IOP doubled from a 14-15 mmHg baseline to an average of 31-34 mmHg during the next 20 minutes of variations. (Personally I was reassured that IOP stabilizes during a long headstand rather than creeping higher and higher.)
He found a similar 100% increase in Adho Mukha Vrksasana (handstand) to 31-34 mmHg, but much smaller increases in Sarvangasana to 16-22 mmHg and in Halasana to 17-18 mmHg. Viparita Karani was measured at 12-14 mmHg, so IOP was stable and even dropped slightly.
He concluded that Sirsasana causes significant IOP elevation, but that IOP returns to normal once upright. For him—and for those without glaucoma—this temporary rise in pressure seems reasonably safe. There’s no proof otherwise, anyway.
But neither he nor the recent researchers make a recommendation either way for those with glaucoma. Perhaps, if glaucoma is managed with drugs or surgery, it doesn’t preclude inversions (or other poses that increase IOP). For those who don’t know they have glaucoma, however, increasing IOP above their already-high IOP might indeed damage the optic nerve.
What poses could you give up?
Ultimately the decision—whether or not to invert—depends on the individual. How risk tolerant or averse are you? What are you willing to continue or to give up, in the face of health risk?
In terms of yoga asana, how much would you miss Sirsasana and other inversions if you had to give them up? While headstand is fundamental to my practice, there are myriad poses and even I, a creature of habit, could adapt to a no-headstand practice. It would be harder for me to give up Adho Mukha Svanasana. In any case, we must remember that yoga is more than poses—and avoid becoming dependent on any pose or habit or way of living.
Images: Rope Sirsasana, Iyengar Yoga Association of Canada; study poses, PLOS ONE; glaucoma, All about Vision.
Acknowledgment: Thanks to WC Sin for sending me the PLOS One article that inspired this post.

Leave a Comment